

Disclaimer
Please note that the following pages are exclusively reserved for health care professionals in countries with applicable health authority product registrations. To the extent this site contains information, reference guides and databases intended for use by licensed medical professionals, such materials are not intended to offer professional medical advice. Prior to use, please consult device labeling for prescriptive information and operating instructions.
Giving LVAD patients with
AR another option.
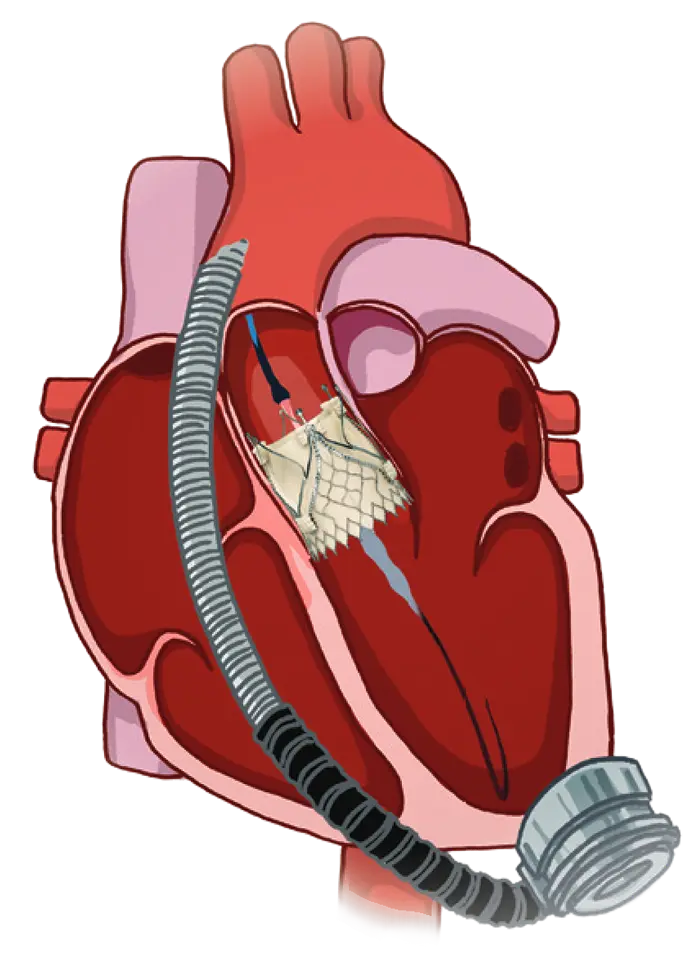
Transcatheter aortic valve replacement (TAVR) using the JenaValve
Trilogy® Heart Valve System for clinically significant aortic regurgitation (AR)
in patients with left ventricular assist devices (LVAD)
Objective and Study Population
JENA-VAD is the first prospective, multi-center clinical registry to evaluate the safety and effectiveness of the JenaValve Trilogy Heart Valve System for TAVR in TAVR-indicated patients with continuous flow left ventricular assist devices (cfLVAD) and clinically significant AR.
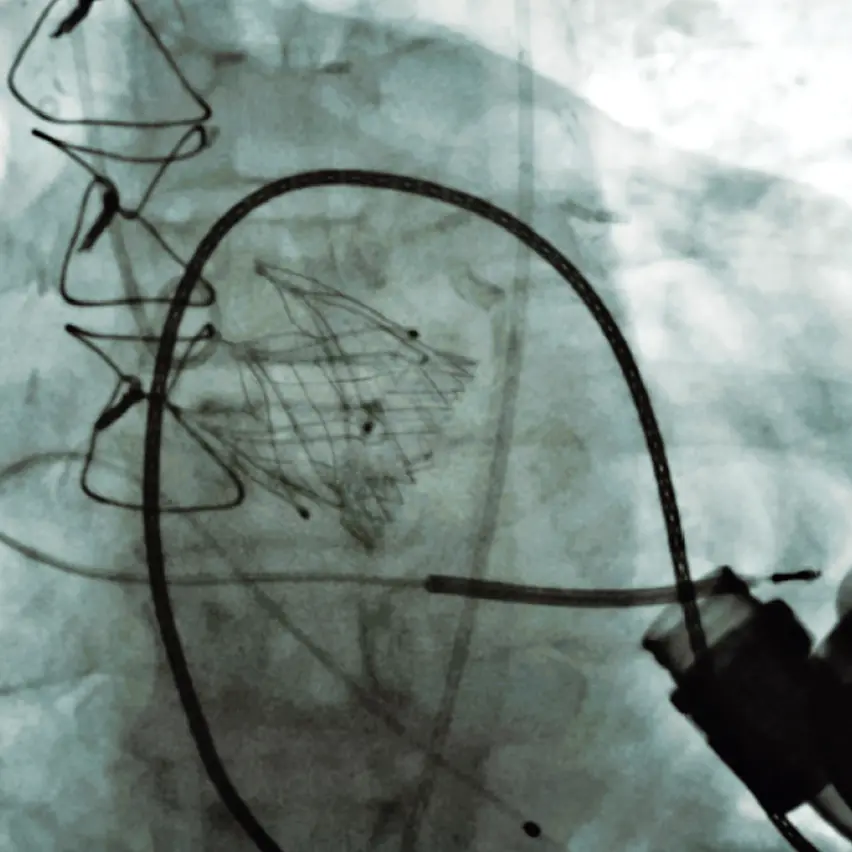
under fluoroscopy
Meeting the Unmet Need
A high-risk population without a
dedicated TAVR solution.

Severe AR in patients with advanced heart failure and LVAD results in recirculation of regurgitant blood volume, for which there is currently no dedicated TAVR solution.
WHY THIS REGISTRY MATTERS
The JENA-VAD registry’s growing body of
clinical evidence opens a new way forward.
STUDY AT A GLANCE
What JENA-VAD studies.
System for the treatment of aortic regurgitation while supported by a cfLVAD.
ELIGIBILITY
Who Is eligible for the registry?
Complete inclusion and exclusion criteria are maintained in the registry protocol.
-
 Adults (>18) with a continuous flow LVAD with clinically significant AR
Adults (>18) with a continuous flow LVAD with clinically significant AR
-
NYHA functional class III or IV
-
Judged at high or greater surgical risk by a multidisciplinary Heart Team
-
Aortic anatomy suitable for the Trilogy device per protocol-defined dimensions
WHAT JENA-VAD MEASURES
Primary outcomes through 1-year follow-up.
For more information
 jena-vad@jenavalve.com
medsci@jenavalve.com
iis@jenavalve.com
jena-vad@jenavalve.com
medsci@jenavalve.com
iis@jenavalve.com
References
1. Goncharov A, et al. EUR Heart J Case Rep. 2023;7:1-6.
POTENTIAL RISKS
Adverse events that may be anticipated in this clinical registry are believed to be consistent with those associated with other minimally invasive surgical and catheter-based procedures, including TAVR procedures. Complications may occur at any time during the procedure, post-procedure or follow-up period.
Potential adverse events (AE) which may be associated with the ancillary procedures including cardiac catheterization, aortic balloon valvuloplasty and local and/or general anaesthesia include but are not limited to the following: vascular damage (e.g. perforation, dissection, contrast media extravasation), vascular access (femoral entry site) complications (e.g. bleeding, hematoma, arteriovenous fistula, arterial occlusion, pseudo aneurysm, wound healing disorder, pain), peripheral nerve injury and/or ischemia, cardiovascular injury (e.g. damage of ventricle, ventricular septal perforation, myocardium or valvular structures including annulus rupture), hypotension, hypertension, cardiogenic tamponade or pericardial effusion, arrhythmias and conduction system disorders (e.g. ventricular tachycardia or fibrillation; AV block) which may require permanent pacemaker implantation, heart murmur, hemodynamic compromise or cardiogenic shock, heart failure or low cardiac output, cardiac arrest, angina pectoris, myocardial infarction, thrombus formation, embolization (e.g. air, calcific material, thrombus), cerebrovascular event (e.g. TIA, stroke, neurologic changes), pulmonary embolism, pulmonary edema, pleural effusion, respiratory compromise or respiratory failure, renal compromise or renal failure, allergic reaction/hypersensitivity to contrast media, medication, or device materials, inflammation, infection (e.g. endocarditis, access site infection) and sepsis, fever, pneumonia, hemorrhage or bleeding, possibly requiring intervention or transfusion, retroperitoneal bleeding, restenosis, syncope, anemia, abnormal laboratory values (e.g. electrolyte imbalance), exercise intolerance or weakness, paralysis, permanent disability, or other comorbid condition (new onset or worsening) or death.

